Nicholasville Nursing and Rehabilitation is excited to shine the spotlight on resident Robert Bryant’s Success Story!
Mr. Bryant was admitted to Nicholasville Nursing and Rehab in August following a brief hospital stay for a UTI. Upon his arrival, he was asking for a walker to walk around his room and was eager to begin therapy to address his deficits in balance, safety, endurance and B UE and LE strength. He worked hard everyday and was walking around the community within days with his rolling walker with limited assist! He was always willing to come to therapy and motivated to participate in all therapy tasks. He is an example of a hard worker, and is returning home to live with his sister in the community, as was his wish upon admission. Good luck, Bob, we know you are going to do great!
Updated guidance reflects new recommendations for isolation and precautions for people with COVID-19.
Removed Assessment for Duration of Isolation and Key Findings From Transmission Literature sections so page provides most current information.
Key Points
People who are infected but asymptomatic or people with mild COVID-19 should isolate through at least day 5 (day 0 is the day symptoms appeared or the date the specimen was collected for the positive test for people who are asymptomatic). They should wear a mask through day 10. A test-based strategy may be used to remove a mask sooner.
People with moderate or severe COVID-19 should isolate through at least day 10. Those with severe COVID-19 may remain infectious beyond 10 days and may need to extend isolation for up to 20 days.
People who are moderately or severely immunocompromised should isolate through at least day 20. Use of serial testing and consultation with an infectious disease specialist is recommended in these patients prior to ending isolation.
Recommendation for Ending Isolation
For people who are mildly ill with SARS-COV-2 infection and not moderately or severely immunocompromised:
Isolation can be discontinued at least 5 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter) if fever has resolved for at least 24 hours (without taking fever-reducing medications) and other symptoms are improving.
Loss of taste and smell may persist for weeks or months after recovery and need not delay the end of isolation.
A high-quality mask should be worn around others at home and in public through day 10. A test-based strategy may be used to remove a mask sooner.
If symptoms recur or worsen, the isolation period should restart at day 0.
People who cannot wear a mask, including children < 2 years of age and people of any age with certain disabilities, should isolate for 10 days.
In certain high-risk congregate settings that have high risk of secondary transmission, CDC recommends a 10-day isolation period for residents.
For people who test positive, are asymptomatic (never develop symptoms) and not moderately or severely immunocompromised:
Isolation can be discontinued at least 5 days after the first positive viral test (day 0 is the date the specimen was collected for the positive test, and day 1 is the next full day thereafter).
A high-quality mask should be worn around others at home and in public through day 10. A test-based strategy may be used to remove a mask sooner.
If a person develops symptoms within 10 days of testing positive, their 5-day isolation period should start over (day 0 changes to the first day of symptoms).
People who cannot wear a mask, including children < 2 years of age and people of any age with certain disabilities, should isolate for 10 days.
In certain high-risk congregate settings that have high risk of secondary transmission, CDC recommends a 10-day isolation period for residents.
For people who are moderately ill and not moderately or severely immunocompromised:
Isolation and precautions can be discontinued 10 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter).
For people who are severely ill and not moderately or severely immunocompromised:
Isolation should continue for at least 10 days after symptom onset (day 0 is the day symptoms appeared, and day 1 is the next full day thereafter).
Some people with severe illness (e.g., requiring hospitalization, intensive care, or ventilation support) may remain infectious beyond 10 days. This may warrant extending the duration of isolation and precautions for up to 20 days after symptom onset (with day 0 being the day symptoms appeared) and after resolution of fever for at least 24 hours (without the taking fever-reducing medications) and improvement of other symptoms.
Serial testing prior to ending isolation can be considered in consultation with infectious disease experts.
Moderately or severely immunocompromised patients may remain infectious beyond 20 days. For these people, CDC recommends an isolation period of at least 20 days, and ending isolation in conjunction with serial testing and consultation with an infectious disease specialist to determine the appropriate duration of isolation and precautions.
The criteria for serial testing to end isolation are:
Results are negative from at least two consecutive respiratory specimens collected ≥ 24 hours apart (total of two negative specimens) tested using an antigen test or nucleic acid amplification test.
Also, if a moderately or severely immunocompromised patient with COVID-19 was symptomatic, there should be resolution of fever for at least 24 hours (without the taking fever-reducing medication) and improvement of other symptoms. Loss of taste and smell may persist for weeks or months after recovery and need not delay the end of isolation.
Re-testing for SARS-CoV-2 infection is suggested if symptoms worsen or return after ending isolation and precautions.
If a patient has persistently positive nucleic acid amplification tests beyond 30 days, additional testing could include molecular studies (e.g., genomic sequencing) or viral culture, in consultation with an infectious disease specialist.
For the purposes of this guidance, moderate to severely immunocompromising conditions include, but might not be limited to, those defined in the interim clinical considerations for people with moderate to severe immunocompromise due to a medical condition or receipt of immunosuppressive medications or treatments.
Other factors, such as end-stage renal disease, likely pose a lower degree of immunocompromise, and there might not be a need to follow the recommendations for those with moderate to severe immunocompromise.
Ultimately, the degree of immunocompromise for the patient is determined by the treating provider, and preventive actions should be tailored to each patient and situation.
Effective September 1st, 2022, CDC Director Rochelle P. Walensky, M.D., M.P.H., endorsed the CDC Advisory Committee on Immunization Practices’ (ACIP) recommendations for use of updated COVID-19 boosters from Pfizer-BioNTech for people ages 12 years and older and from Moderna for people ages 18 years and older.
Updated COVID-19 boosters add Omicron BA.4 and BA.5 spike protein components to the current vaccine composition, helping to restore protection that has waned since previous vaccination by targeting variants that are more transmissible and immune-evading.
In the coming weeks, CDC also expects to recommend updated COVID-19 boosters for other pediatric groups, per the discussion and evaluation of the data by ACIP on Sept. 1, 2022. When data are available and FDA authorizes these other types of COVID-19 boosters, CDC will quickly move to help make them available in the United States.
The Food and Drug Administration’s (FDA) authorization of updated COVID-19 boosters, and CDC’s recommendation for use, are critical next steps forward in our country’s vaccination program—a program that has helped provide increased protection against COVID-19 disease and death.
The following is attributable to Dr. Walensky:
“The updated COVID-19 boosters are formulated to better protect against the most recently circulating COVID-19 variant. They can help restore protection that has waned since previous vaccination and were designed to provide broader protection against newer variants. This recommendation followed a comprehensive scientific evaluation and robust scientific discussion. If you are eligible, there is no bad time to get your COVID-19 booster and I strongly encourage you to receive it.”
CDC works 24/7 protecting America’s health, safety and security. Whether disease start at home or abroad, are curable or preventable, chronic or acute, or from human activity or deliberate attack, CDC responds to America’s most pressing health threats. CDC is headquartered in Atlanta and has experts located throughout the United States and the world.
Number of Shots: 2 doses in the primary series, given 3–8 weeks apart.
People who are moderately or severely immunocompromised should also receive 2 doses, given 3 weeks apart (a 3rd primary dose is not currently authorized).
Booster Shot: Novavax COVID-19 vaccine is not authorized for use as a booster dose.
COVID-19 vaccines have undergone—and continue to undergo—the most intensive safety monitoring in U.S. history. Side effects that happen within 7 days of getting vaccinated are common but are mostly mild and only last a few days. Some people have reactions that affect their ability to do daily activities.
Side effects throughout the body (such as fever, chills, tiredness, and headache) are more common after the second dose of the vaccine.
Severe allergic reactions to vaccines are rare but can happen. Cases of myocarditis and pericarditis have been reported in people who received Novavax COVID-19 vaccine.
Vaccines reduce the risk of COVID-19, including the risk of severe illness and death among people who are fully vaccinated.
COVID-19 vaccines are effective. Clinical trials demonstrate that Novavax COVID-19 reduces the risk of COVID-19, including the risk of severe illness and death. However, studies from other COVID-19 vaccines have shown that protection declines over time especially with the Omicron variant.
All FDA-approved or authorized COVID-19 vaccines provide substantial protection against COVID-19 hospitalization and death.
CDC will continue to provide updates as we learn more.
COVID-19 vaccine ingredients are considered safe for most people. Nearly all of the ingredients in COVID-19 vaccines are ingredients found in many foods—fats, sugar, and salts. The Novavax COVID-19 vaccine also includes harmless pieces (proteins) of the virus that causes COVID-19; they are pieces of what is often called the spike protein. After vaccination, the body creates an immune response to these protein pieces. This response helps protect you from getting sick with COVID-19 in the future. After the body produces an immune response, it discards all the vaccine ingredients, just as it would discard any substance that cells no longer need. This process is a part of normal body functioning.
All COVID-19 vaccines are manufactured with as few ingredients as possible and with very small amounts of each ingredient. Each ingredient in the vaccine serves a specific purpose as seen in the table below.
Type of Ingredient
Ingredient
Purpose
Protein
SARS-CoV-2 recombinant spike protein
Causes an immune response that helps protect the body from getting sick with COVID-19 in the future.
Lipids (fats)
Cholesterol Phosphatidylcholine
Work together to help the recombinant spike protein enter cells
Adjuvant
Fraction-A and Fraction-C of Quillaja saponaria Molina extract.
Facilitates activation of the cells of the innate immune system.
Work together to help keep the vaccine molecules stable while the vaccine is manufactured, shipped, and stored until it is ready to be given to a vaccine recipient.
The vaccine may also contain very small amounts of ingredients from the manufacturing stage, which can be found in the EUA Fact Sheet.
INGREDIENTS THAT ARE NOT USED IN COVID-19 VACCINES
The above table lists ALL ingredients in the Novavax COVID-19 vaccine. There are NO ingredients in this vaccine beyond what is listed in the table. The Novavax COVID-19 vaccine has:
No preservatives such as thimerosal or mercury or any other preservatives.
No antibiotics such as sulfonamide or any other antibiotics.
No medicines or therapeutics such as ivermectin or any other medications.
No tissues such as aborted fetal cells, gelatin, or any materials from any animal.
No food proteins such as eggs or egg products, gluten, peanuts, tree nuts, nut products, or any nut byproducts (COVID-19 vaccines are not manufactured in facilities that produce food products).
No metals such as iron, nickel, cobalt, titanium, rare earth alloys, or any manufactured products like microelectronics, electrodes, carbon nanotubes or other nanostructures, or nanowire semiconductors.
No latex. The vial stoppers used to hold the vaccine also do not contain latex.
Learning about how COVID-19 spreads and the factors that can increase or decrease that risk can help you make informed choices.
The questions below are written in past tense to help you assess the likelihood that you were infected when you were around a person with COVID-19. If multiple factors below indicate higher transmission risk, you should follow the steps for what to do if you are exposed.
You can also ask yourself the same questions, but about future interactions with others, to help you decide what prevention actions to take. If multiple factors below indicate higher transmission risk, you should consider adding more prevention actions.
Factors that lower or increase risk of transmission
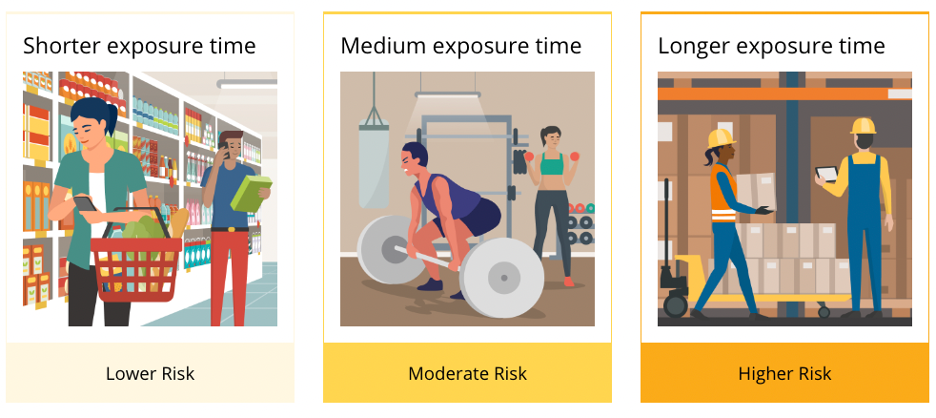
Length of time: How long were you with the infected person?
Longer exposure time increases the risk of transmission (for example, contact longer than 15 minutes is more likely to result in transmission than two minutes of contact).
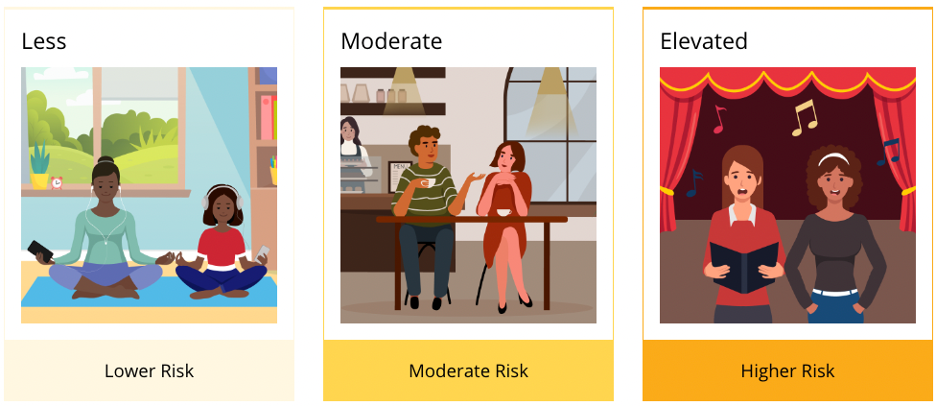
Cough or heavy breathing: Was the infected person coughing, singing, shouting, or breathing heavily?
Activities like coughing, singing, shouting, or breathing heavily due to exertion increase the risk of transmission.
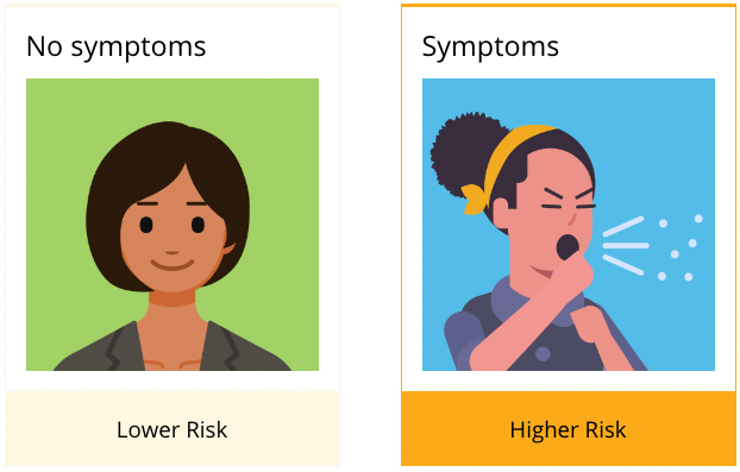
Symptoms: Did the infected person have symptoms at the time?
Being around people who are symptomatic increases the risk of transmission.
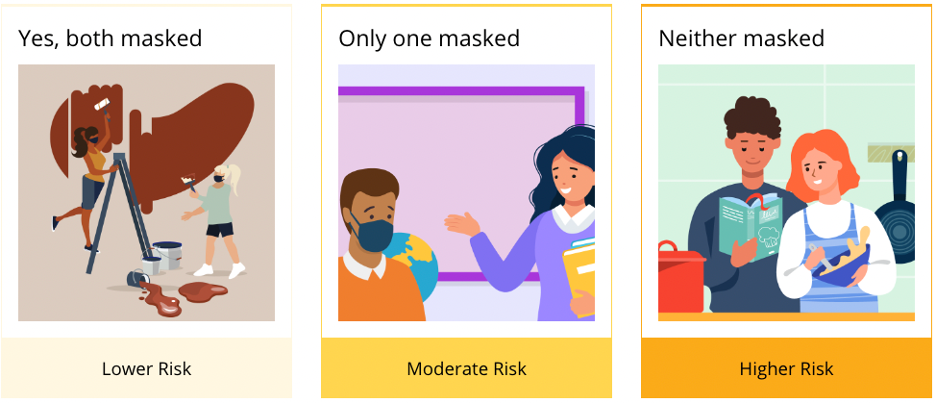
Masks: Were you or the infected person or both wearing a respirator (for example, N95) or high-quality mask?
If one person was wearing a mask, the risk of transmission is decreased, and if both people were wearing masks, the risk is substantially decreased. Risk is also lower if the mask or respirator is a type that offers greater protection.
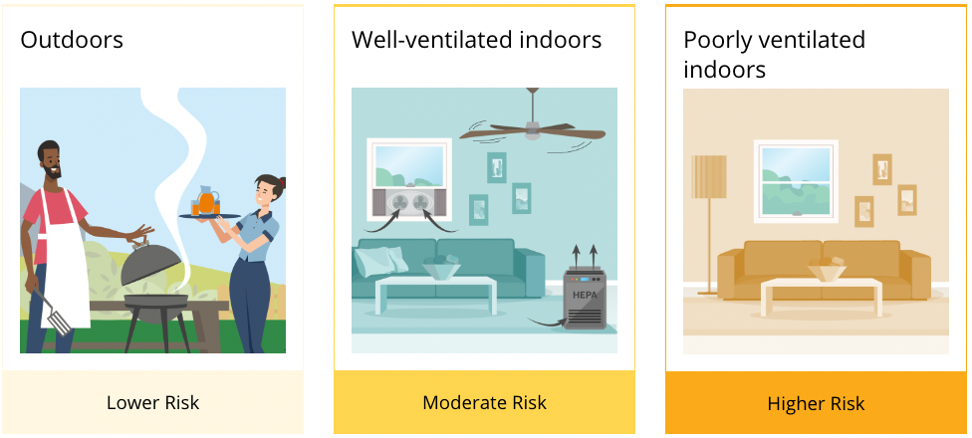
Ventilation and filtration: How well-ventilated was the space?
More outdoor air can decrease the risk of transmission. Being outside would be lower exposure risk than being indoors, even with good ventilation and filtration; both of those options would be lower risk than being indoors with poor ventilation or filtration. See the Interactive Home Ventilation Tool.
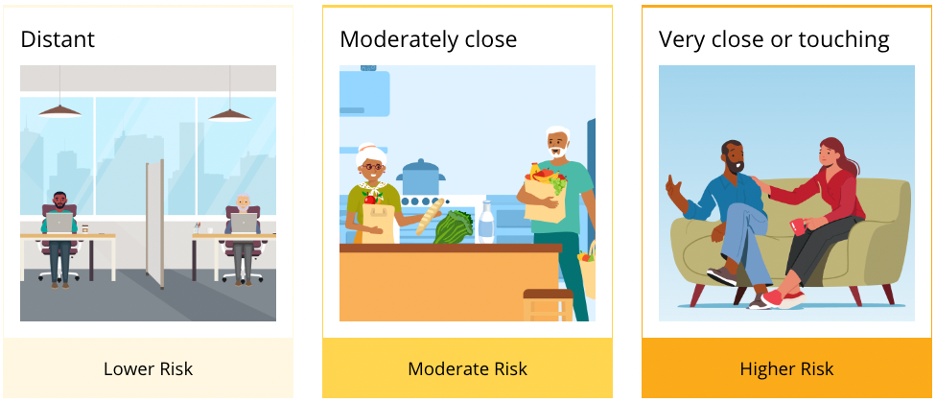
Distance: How close was the infected person to you?
Being closer to someone who is infected with COVID-19 increases the risk of transmission. Crowded settings can raise your likelihood of being close to someone with COVID-19.
The benefits of COVID-19 vaccination continue to outweigh any potential risks.
CDC is providing timely updates on the following adverse events of interest:
Anaphylaxis after COVID-19 vaccination is rare and has occurred at a rate of approximately 5 cases per one million vaccine doses administered. Anaphylaxis, a severe type of allergic reaction, can occur after any kind of vaccination. If it happens, healthcare providers can effectively and immediately treat the reaction. Learn more about COVID-19 vaccines and allergic reactions, including anaphylaxis.
CDC scientists have conducted detailed reviews of cases of anaphylaxis and made the information available to healthcare providers and the public:
Thrombosis with thrombocytopenia syndrome (TTS) after J&J/Janssen COVID-19 vaccination is rare and has occurred in approximately 4 cases per one million doses administered. TTS is a rare but serious adverse event that causes blood clots in large blood vessels and low platelets (blood cells that help form clots).
A review of reports indicates a causal relationship between the J&J/Janssen COVID-19 vaccine and TTS. CDC scientists have conducted detailed reviews of TTS cases and made the information available to healthcare providers and the public:
Guillain-Barré Syndrome (GBS) in people who have received the J&J/Janssen COVID-19 vaccine is rare. GBS is a rare disorder where the body’s immune system damages nerve cells, causing muscle weakness and sometimes paralysis. GBS has largely been reported in men ages 50 years and older.
Based on a recent analysis of data from the Vaccine Safety Datalink, the rate of GBS within the first 21 days following J&J/Janssen COVID-19 vaccination was found to be 21 times higher than after Pfizer-BioNTech or Moderna (mRNA COVID-19 vaccines). After the first 42 days, the rate of GBS was 11 times higher following J&J/Janssen COVID-19 vaccination. The analysis found no increased risk of GBS after Pfizer-BioNTech or Moderna (mRNA COVID-19 vaccines). CDC and FDA will continue to monitor for and evaluate reports of GBS occurring after COVID-19 vaccination and will share more information as it becomes available.
Myocarditis and pericarditis after COVID-19 vaccination are rare. Myocarditis is inflammation of the heart muscle, and pericarditis is inflammation of the outer lining of the heart. Most patients with myocarditis or pericarditis after COVID-19 vaccination responded well to medicine and rest and felt better quickly. Most cases have been reported after receiving Pfizer-BioNTech or Moderna (mRNA COVID-19 vaccines), particularly in male adolescents and young adults.
A review of vaccine safety data in VAERS from December 2020–August 2021 found a small but increased risk of myocarditis after mRNA COVID-19 vaccines. Over 350 million mRNA vaccines were given during the study period and CDC scientists found that rates of myocarditis were highest following the second dose of an mRNA vaccine among males in the following age groups:
12–15 years (70.7 cases per one million doses of Pfizer-BioNTech)
16–17 years (105.9 cases per one million doses of Pfizer-BioNTech)
18–24 years (52.4 cases and 56.3 cases per million doses of Pfizer-BioNTech and Moderna, respectively)
Multiple studies and reviews of data from vaccine safety monitoring systems continue to show that vaccines are safe. As a result, the agency will refocus enhanced surveillance and safety monitoring efforts toward children and adolescents.
As of July 28, 2022, there have been 1,010 preliminary reports in VAERS among people younger than age 18 years under review for potential cases of myocarditis and pericarditis. Of these, 258 remain under review. Through confirmation of symptoms and diagnostics by provider interview or review of medical records, 665 reports have been verified to meet CDC’s working case definition for myocarditis. See below for counts of verified reports of myocarditis by age group.
5-11 years: 22 verified reports of myocarditis after 20,404,074 doses administered
12-15 years: 346 verified reports of myocarditis after 24,198,309 doses administered
16-17 years: 297 verified reports of myocarditis after 13,326,016 doses administered
Reports of death after COVID-19 vaccination are rare. FDA requires healthcare providers to report any death after COVID-19 vaccination to VAERS, even if it’s unclear whether the vaccine was the cause. Reports of adverse events to VAERS following vaccination, including deaths, do not necessarily mean that a vaccine caused a health problem. More than 603 million doses of COVID-19 vaccines were administered in the United States from December 14, 2020, through July 27, 2022. During this time, VAERS received 15,700 preliminary reports of death (0.0026%) among people who received a COVID-19 vaccine. CDC and FDA clinicians review reports of death to VAERS including death certificates, autopsy, and medical records.
Continued monitoring has identified nine deaths causally associated with J&J/Janssen COVID-19 vaccination. CDC and FDA continue to review reports of death following COVID-19 vaccination and update information as it becomes available.
Nicholasville Nursing and Rehabilitation is excited to share resident Eugenia Morgan’s Success Story!
Mrs. Morgan was admitted to our community on August 2nd of last year for overall general weakness. In order to return home, she had to improve her functional independence. Mrs. Morgan participated in physical, occupational, and speech therapy in order to target ambulation, balance, activities of daily living, and cognitive function. Mrs. Morgan had excelled in all aspects and had demonstrated functional abilities to discharge back into her home with her family! It has been nothing short of a pleasure to work with Mrs. Morgan. Congratulations to her and her Care team on their success!
The Novavax COVID-19 vaccine is a protein subunit COVID-19 vaccine that is authorized for use in the United States under Emergency Use Authorization. Learn more about Novavax COVID-19 vaccine, including who can get it, doses, and ingredients.
How Protein Subunit COVID-19 Vaccines Work
Protein subunit vaccines contain pieces (proteins) of the virus that causes COVID-19. These virus pieces are the spike protein. The vaccine also contains another ingredient called an adjuvant that helps the immune system respond to that spike protein in the future. Once the immune system knows how to respond to the spike protein, the immune system will be able to respond quickly to the actual virus spike protein and protect you against COVID-19.
First, protein subunit COVID-19 vaccines are given in the upper arm muscle. After vaccination, nearby cells pick up these proteins.
Next, our immune system recognizes that these proteins do not belong there. Another ingredient in the vaccine, the adjuvant, helps our immune system to produce antibodies and activate other immune cells to fight off what it thinks is an infection. This is what your body might do if you got sick with COVID-19.
At the end of the process, our bodies have learned how to help protect against future infection with the virus that causes COVID-19. The benefit is that people get this protection from a vaccine, without ever having to risk the potentially serious consequences of getting sick with COVID-19. Many side effects from getting the vaccine are normal signs the body is building protection.
Facts About Protein Subunit COVID-19 Vaccines
Protein subunit COVID-19 vaccines cannot cause COVID-19 or other illnesses.
Protein subunit COVID-19 vaccines do not use any live virus.
Protein subunit COVID-19 vaccines cannot cause infection with the virus that causes COVID-19 or other viruses.
They do not affect or interact with our DNA.
The protein pieces do not enter the nucleus of the cell where our DNA (genetic material) is located, so they cannot change or influence our genes.
Protein Subunit COVID-19 Vaccines Have Been Rigorously Evaluated for Safety
Protein subunit COVID-19 vaccines have been held to the same rigorous safety and effectiveness standards as all other types of vaccines in the United States. The only COVID-19 vaccines the Food and Drug Administration (FDA) makes available for use in the United States (by approval or emergency use authorization) are those that meet these standards.
Protein Subunit Vaccines Have Been Used for Years
More than 30 years ago, a hepatitis B vaccine became the first protein subunit vaccine to be approved for use in people in the United States. Another example of other protein subunit vaccines used in the United States today include acellular pertussis (whooping cough) vaccines.
To learn more, please visit https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/proteinsubunit.html
Nicholasville Nursing and Rehabilitation is excited to shine the spotlight on resident Linda Burchell’s Success Story!
Linda was admitted to Nicholasville Nursing and Rehabilitation on June 9, 2022 after being hospitalized a second time with COVID-19. She was initially very weak and unable to get out of bed, or ambulate on her own. She required extensive assist to perform basic activities of daily living. She was highly motivated to return to her home alone and worked hard every day in therapy with Occupational and Physical Therapy to address her deficits in balance, safety, activity tolerance and overall strength. Within three weeks, she was able to make significant progress and complete all daily living tasks and was able to ambulate up to 100 feet with a rolling walker! She was eager to return home and we are so proud of all of her hard work. Way to go, Linda!
COVID-19 vaccines help protect against severe illness, hospitalization and death. COVID-19 vaccines also help protect against infection. People who are vaccinated may still get COVID-19. When people who have been vaccinated get COVID-19, they are much less likely to experience severe symptoms than people who are unvaccinated.
When someone who is vaccinated with either a primary series or a primary series plus a booster dose gets infected with the virus that causes COVID-19, it is referred to as a “vaccine breakthrough infection.”
When people who are vaccinated get COVID-19 get a breakthrough infection, they are much less likely to experience severe symptoms than people who are unvaccinated.
People who get vaccine breakthrough infections can spread COVID-19 to other people. When a community reports more COVID-19 infections, that means more virus is circulating. When more virus is circulating, more breakthrough infections will occur even when vaccination rates are high. Even if you are vaccinated, if you live in a county with a high COVID-19 Community Level, you and others in your community, whether vaccinated or not, should take more steps to protect yourself and others, like wearing a mask in indoor public places.
CDC monitors reported vaccine breakthrough infections to better understand patterns of COVID-19 among people who are vaccinated and unvaccinated. The latest rates of COVID-19 cases and deaths by vaccination status are available on the CDC COVID Data Tracker.
To learn more, please visit https://www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/why-measure-effectiveness/breakthrough-cases.html
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.